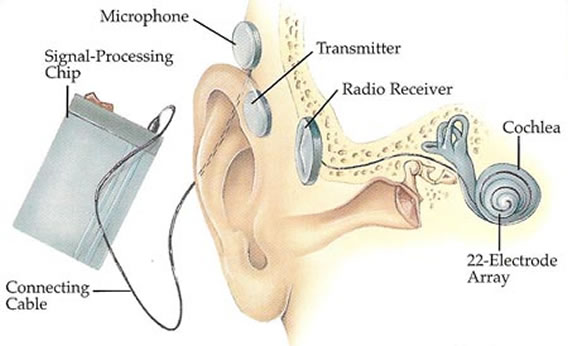
→The different components of cochlear implant are:
- Internal part (implant): placed surgically beneath the scalp
- Array of electrode inside cochlea
- Body of implant which contains a receiver/stimulator: decodes the signals from the external prosthesis and send the electrical charges to the individual electrodes.
- External part:
- Microphone
- Speech processor
- Transmitting coil
→The two main strategies used:
I. Continuous interleaved sampling (CIS): Med-EL(TM) and Clarion (TM)
II. Spectral peak processing (SPEAK): Cochlear(TM)
The patient selection criteria for cochlear transplant surgery have evolved over times as advances in cochlear implant technology produced subsequent improvement in performance outcomes. At any point, however, candidacy resolves around three basic questions:
- Is physical implantation of the device possible and/or advisable given the medical status of the patient?
- Is it likely that an individual will receive more communication benefit from a cochlear implant than from a hearing aid or alternatively, from no hearing prosthesis at all?
- Do the necessary supports exit in the individual psychological, family, education and rehabilitative situation to keep a cochlear implant working and integrate into the patient’s life? If not, can they be developed?
Initially, only individuals with bilateral profound SNHL with no open set speech recognition were considered candidates for cochlear implants.
[table id=17 /]
The evaluation of candidacy process is a team approach:
- Audiologist
- Speech and language specialists
- Social worker
- Education consultant operating surgeon
ADULTS:
- Individual 18 years of age or older
- Severe to profound sensorineural hearing loss in both ears.
- Recently individuals with mild to moderate low frequency hearing with absent high frequencies are considered candidates for cochlear implantation using EAS.
- 2- speech recognition scores:
- Advanced bionics specified sentence recognition up to 50% in the best aided condition.
- Cochlear specified sentence recognition up to <50% sentence recognition in the ear to be implanted and <=60% in the opposite ear or binaurally, in the best aided condition.
- Med El listed sentences recognition up yo 40% correct in the best aided condition.
CHILDREN (2-17 years)
- Severe to profound sensorineural hearing loss
- Limited benefit from binaural amplification.
- Multi-syllabic Lexical Neighborhood Test (MLNT) or Lexical Neighborhood Test (LNT) scores <=30%.
- FDA preimplant word recognition performance candidacy criteria for older children ranges range from 12-30% correct in the best aided condition.
- During the hearing aid trial (3 months period, children should be making at least month to month auditory progress as well as speech and language developmental progress.
- Regular speech therapy should be considered a part of the hearing aid trial for all children being seen for implant evaluation.
Children(12-24 months)
- B/I Profound sensorineural hearing loss
- Child must weigh about 9-10 kg from an anaesthesia viewpoint.
- Limited benefit from binaural amplification
- Specific circumstances may allow for earlier implantation. A child with meningitis is implanted as early as possible as the condition causes cochlear ossification. It also help to decrease the duration of auditory deprivation and its deleterious effects on the auditory pathways.
OTHER CANDIDACY CRITERIA:
- Family willingness to follow recommendations: enroll in speech, language and auditory therapy; and return from the follow up appointments.
- Educational and home environments that is supportive of cochlear implants
- Having no medical contraindications to electrode insertion or receiver placement. Otitis media must be diagnosed and managed prior to implantation.Prior ear or prosterior fossa surgery must be investigated preoperatively.
The candidates can be divided into three categories. Among these, change over at an earlier age candidates make excellent implants as some plasticity for articulation still remains.
[table id=18 /]
Post lingual category can be divided into:
- Post pubertal: adults and teenager who becomes deaf after experiencing normal hearing during their childhood and they are excellent candidates.
- Prepubertal group: 2-12 years and younger the child more likely speech will be lost.
In cochlear implant systems, the channel refers to the number of stimulation sites within the inner ear, or cochlea, and is defined by a range of frequencies or pitches. All sounds, ranging from low pitch (bass) to high pitch (treble) sound are separated into the number of available channels. The advantages of multi channel over single channel cochlear implant are:
[table id=19 /]

