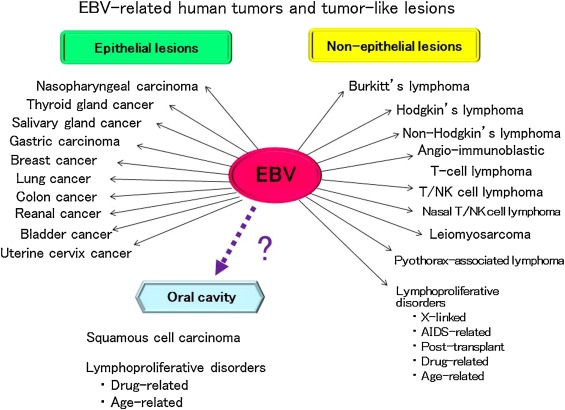
- EBV is one of the herpes viruses and B cell lymphotrophic.
- The primary infection of EBV takes place in childhood and is always accompanied by seroconversion and harboring of the virus in a dormant state for life in small numbers of circulation B lymphocytes or in saliva.
- The virus may be reactivated with raised serological titres in immunodeficient states.
- More than 90% of patients with Nasopharyngeal Carcinoma have elevated titers of EVM determined antigens, particularly IgA class.
- Of the many types NPC, only the undifferentiated /poorly differentiated carcinomas have immunocytological association with EBV.
- Epithelial cells are infected by EBV, whether it is before or after the malignant change (passenger virus),or as a result of impaired host immunity. EBV transform B lymphocytes but there is no convincing evidence at present that it can transform epithelial cells.
- EBV itself doesn’t replicate in NPC tumours cells and its viral antigens (VGA and EA) are not expressed in these tumours.
EBV Serological markers
Important EBV related antibodies in NPC are
- IgA and IgG to viral capsid (VCA)
- IgA and IgG to early antigen (EA)
- Antibody to nuclear antigen(EBNA)
- Antibody dependent cellular cytotoxicity antibodies
These are important for:
- diagnosis
- evaluation of effect and response to therapy
- evaluation of clinical courses and survival
- Prognosis
- screening
VCA/EA/NA are most useful in clinical practical and their fitres correlate well with each other.
Diagnosis
- IgA response to EBV antigens in NPC is unique and characteristics of patient NPC.
- Sensitivity of IgA /VCA →95%
- Specification of IgA /VCA →97%
- Sensitivity of IgA /EA →90%
- Specification of IgA /EA →99%
Clinical Course and survival(Post radiotherapy)
The titres of IgA /VCG and TgA /EA are useful clinical indices for F/U of patient after treatment.
It declines to a low level or remain static after successful treatment.
If (VCA,EA,EBNA) antibodies increase it indicates clinical recurrence and/or metastasis. Thus necessitate careful evaluation of patient.
ADCC antibody titre α long term survival whereas VCA and EA ½ α survival.
Prognostic markers
The prognostic makers of NPC include specific EBV antibody tires.
The EBV tires are dependent on the histological type, the viral antigen load and host immune competence
The titres may not be elevated in early and end stage disease and in patient c intracranial extension without significant lymphnode involvement.
- Prognosis and survival are 1/α the geometric mean titres of VCA and EA antibodies.
- Good prognosis is indicated by high ADCC antibody tires.
Screening of NPC in high populations
IgA/VCA is of practical value in serological screening for NPC in endemic regions. A raised IgA /VCA titre identifies those high risk individuals for futher clinical and immuno-histological evaluation of the nasopharynx.

